

KKOH provides extensive patient resources and educational materials to help patients understand their conditions, treatments, and recovery processes. Our patient education program empowers individuals to actively participate in their healthcare decisions and achieve optimal outcomes through informed choices.
Educational resources are available in multiple formats including printed materials, digital guides, video
demonstrations, and interactive sessions with healthcare professionals. All materials are designed to be easily understood while providing comprehensive information about orthopedic conditions and treatments.
The patient education approach recognizes that informed patients achieve better outcomes and experience less anxiety about their treatment. Our resources address common questions, concerns, and misconceptions while providing practical guidance for managing orthopedic conditions effectively.

Total Knee Replacement (TKR) is called Total Knee Arthroplasty (TKA) is a surgery done for damaged knee where the surface of the bones that join in the knee are replaced. The damage to the joint surface produces severe pain and or deformity. There are three components which replace the worn out surfaces of the knee joint. The distal end of femur, the thigh bone is replaced with a femoral component and the upper end of tibial, the leg bone is replaced with a tibial component. A polythene is inserted in between the two in a way that movement occurs between the femoral component and the polythene, therefore there is no pain.The tibial and femoral components are firmly fixed to the bone with a material called bone cement. There are techniques to fix the components to the bone with out bone cement, but cement fixation is highly recommended.
This is a time tested surgery had its origin some time in the 1970s. Lot of modifications were done subsequently in the components and the technique of fixation. Today this is one of the promising surgeries for damaged knee.
There are many companies marketing the knee joint components some Indian, some imported. The femoral and tibial components could be made of cobalt chrome stainless steel or titanium. Titanium is more bio compatible.
The surgery is done usually under spinal anaesthesia, post operative pain is managed by regional nerve block combined with pain medications. Usually the patient is made to walk with support on the second or third day. Knee bending exercises are started on the third day. Maximum knee flexion obtained after surgery is about 90 degrees. Patient is advised not the squat or sit cross legged. All other activities like walking, climbing stairs, travelling are permitted after 3 months after surgery.
Surgery can be done on both knees in a single sitting or on different days in the same admission or on different times as preferred by the patient and anaesthetic clearance.
The most important complications of TKA are infection and aseptic loosening of the components. At KKOH, special care is taken to prevent this. Our infection rate is much lower than international standards. Aseptic loosening usually occurs in knee with rheumatoid arthritis. All patients undergoing TKA have a bone density scanning done to assess the bone strength so that the chances of this complication could be minimised.
Robotic assisted TKA is a relatively new concept where the robot assists the surgeon in getting the ideal bone cuts. The advantage is that it adds precision to the surgery. The disadvantage is that the choice of the implants gets limited to that of only company. This deprives the surgeon of the choice of the company depending on the specific need of Individual patient. The results are highly surgeon dependent. Robotic assisted TKA also needs further long term studies to establish its superiority.
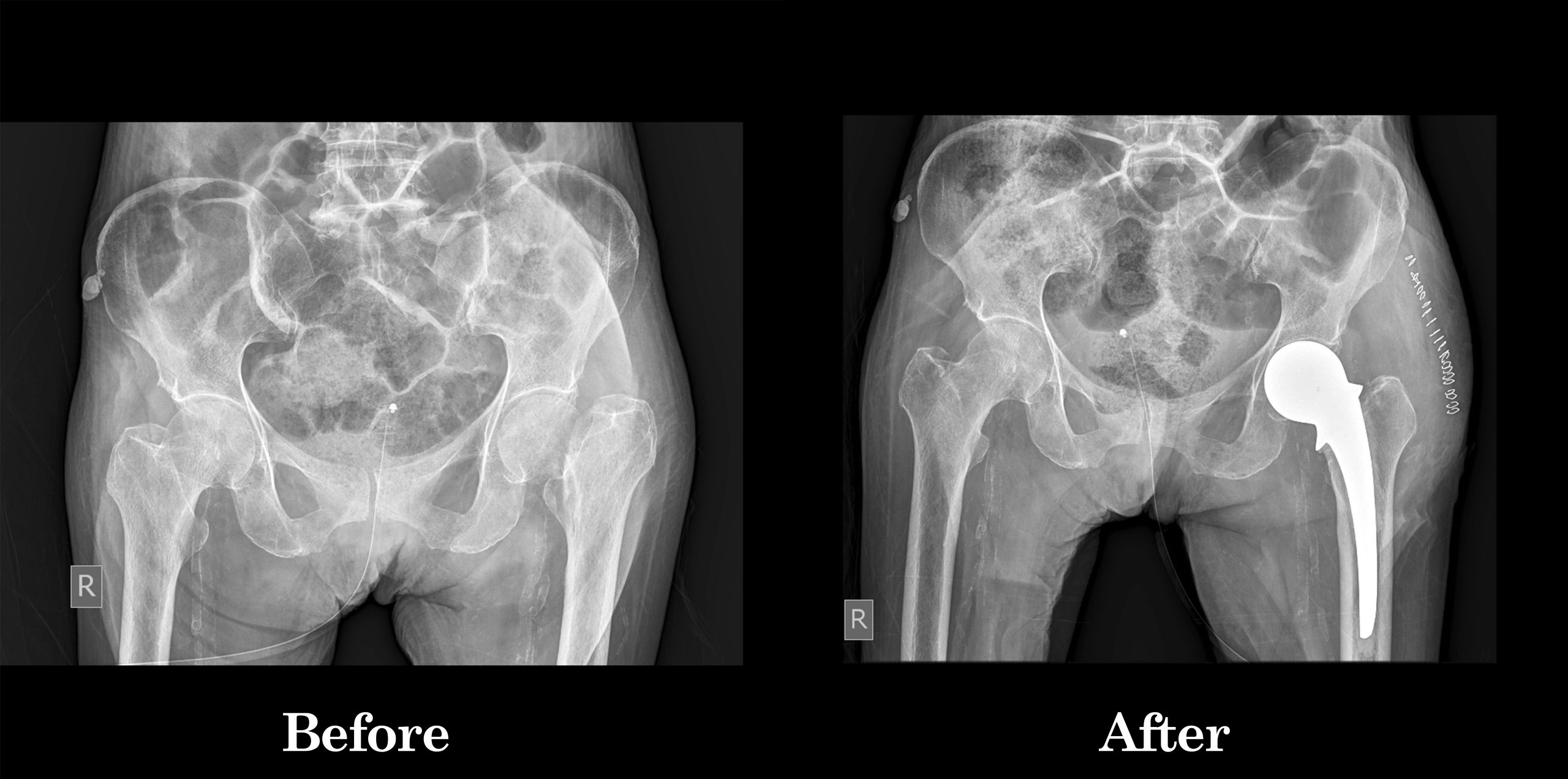
This is a surgery where both the ball and socket of the hip joint are replaced with artificial materials.
The normal hip joint consists of a cup called the acetabulum into which articulates a head of the thigh bone called the femur.
This joint may become damaged due to a variety of conditions. The common causes are rheumatoid arthritis, ankylosing spondylitis, childhood diseases like perches, injury to the hip joint etc. There is loss of articular cartilage, a smooth lining of the ends of the bone in a joint. The result is that raw bones rub against each other causing pain. This condition where the articular cartilage is damaged, is collectively called arthritis.
Damage to hip joint can occur at any age. Total hip replacement can be done after the age of 20 years.
There are three basic components in a total hip system. The stem which is into the medullary cavity of the femur bone. The head which is fixed to the stem and cup which is fixed to the acetabulum. The acetabular component may be only of polythene material or a titanium shell which holds the polythene cup.
There are two basic types of total hip system, the cemented and the uncemented. In the cemented system, the components are fixed to the bone by a material called bone cement which firmly fixes the components to the bone. The uncemented total hip system does not use cement for fixation, instead rely on firm fixation by scratch fit.
There are various materials by which the head and the cup are made of. The older version is a stainless-steel head articulating with a polyethylene cup. In this type of articulation, the head rubs against the polyethylene cup and gets worn out faster. The particles so generated by the wear of polyethylene will cause damage to the bone which can cause loosening of the components from the bone, a condition called aseptic loosening. To avoid this, complication, various other material combinations are available. Ceramic is a promising material. The ceramic cup with ceramic head is long lasting. Ceramic head can also be coupled with polyethylene cup which also gives comparable long-term results. On an average, these materials are designed to last for more than 20 years.
The surgery is done usually under spinal anesthesia. Through a surgical exposure, the damaged head of femur is removed, the acetabulum is reamed to make the surface rough so that the hold of the artificial cup is better. After the cup and stem with the head are implanted, the patient is kept under observation for a day or two in the post operative ward. A drain may be inserted in the wound during surgery to drain the blood that may collect in the wound. This step is an attempt to prevent infection. The drain is usually removed on the 2nd post operative day. The patient may be given some antibiotics and blood thinning agents. In the normal course, the patient can start standing and walking with support by the end of 4th post operative day. In the first few days, pain relievers are given. He is usually discharged on the 5th post operative day. He comes back after 10 days for suture removal.
There are a few potential complications in total hip replacement surgery. In the first two or three days after surgery, patient may develop clotting of blood in the leg veins. Occasionally, this blood clot may travel in the blood to get lodged in the lungs. The patients are given blood thinning agents to prevent this complication. DVT stocking and calf muscle pumps can also prevent this complication.
Post operative Infection is another complication, every step is taken to prevent this. At KKOH, strict sterilization and aseptic procedures are carried out. Our infection rate is very low compared to international standards.
Total hip replacement is usually a promising surgery if done by an experienced surgeon taking adequate precautions.
Most patients, even after major surgeries get discharged in a few days after surgery. The advantages of short hospital stay are, patients and relatives feel psychologically comfortable at home and the hospital cost could be substantially reduced. It has been proved that the chances of surgical site infection is less with early discharge.
But there are some patients, like old people, very small children, patients who are advised not weight bearing and people who need supervised physiotherapy need continued support.
Home care support is given by qualified staff and physiotherapists at the home of the patient after discharge from the hospital. Regular dressing, physiotherapy, walking training are provided by KKOH staff at the residence
of the patient. This service is available only for patients within the reach of KKOH, in and around Nagercoil. Only supportive services are given. Total care of the patients at their home (home nursing) is not done by KKOH. Ambulance services to shift the patient from hospital to home and from home to hospital for review can also be arranged.
Our state-of-the-art facility combines advanced medical technology with compassionate care, making us the preferred choice for patients seeking specialized bone and joint treatment.
Copyright © 2026 KRISHNAKUMAR ORTHOPAEDIC HOSPITAL AND Private Limited Company – All rights reserved. Powered by Demanzo